
SYNOVIAL PLICA, BURSITIS, AND ILIOTIBIAL
BAND FRICTION SYNDROME

Synovial plicae are folds of embryonic remnants of the synovial membrane. In the fetus, thin synovial membranes divide the knee joint into three compartments (medial, lateral, and patellar). In the fifth month of fetal development, these partitions usually degenerate and the knee joint becomes one cavity. Incomplete degeneration of one or more of the membranes can result in the formation of plicae. Most synovial folds contain a considerable amount of elastin and areolar tissue and are thus extensible and asymptomatic. Many are detected during routine arthroscopic procedures performed for other reasons.
Plicae can be found anywhere in the knee joint, but
the most common location is over the medial femoral condyle. Folds in this
location are called medial, or shelf, plicae. This is the area most susceptible
to trauma and subsequent irritation. When the knee is extended, the patella
protects the anterior aspect of the femoral condyles, but when the knee is
flexed, the medial condyle is more vulnerable. Multiple traumatic events, even
minor ones, that involve the condyle, repeated flexion-extension activities, or
direct contusions can lead to inflammation of the plica with subsequent
thickening. The thickened plica may cause local irritation and erosion of the
underlying hyaline cartilage on the condyle. The symptoms of a pathologic plica
may mimic those of a torn meniscus. Patients may complain of mechanical
symptoms (snapping or clicking), along with pain along the medial joint line.
Physical Examination and Special Tests
1.
Plica tests: The patient is supine and relaxed. With the tibia internally rotated,
the examiner passively flexes and
extends the knee from 30 to 100 degrees of flexion. Examining fingers placed
along the medial patellofemoral joint may feel a click, possibly some
tenderness, or even a pop of a pathologic plica.
Imaging. Diagnosis can
be confirmed by doublecontrast arthrography of the knee joint. MRI is also
routinely available for these patients as part of the diagnostic workup for
their painful knee.
Treatment. Initially,
symptomatic plicae should be managed with rest from activities that irritate
the knee, use of nonsteroidal anti-inflammatory drugs (NSAIDs), and application
of ice. In patients whose knees do not improve with nonoperative treatment,
arthroscopic excision can be very effective. If plicae are an incidental finding
on arthroscopy, it is up to the surgeon to determine whether excision would be beneficial based on the patient’s
symptomology.
Inflammation may occur at any of the many bursae
around knee, usually evidenced by swelling and pain. Typically, the prepatellar
bursa, pes anserinus bursa, tibial collateral ligament bursa, and deep
infrapatellar bursa are involved. This is usually the result of overuse but may
be due to a direct blow with bleeding into a bursa. Septic bursitis with entrance
of infectious organ- ism may also be encountered and may present as other
systemic signs of infection. Careful physical examination and routine
laboratory studies, such as a white blood cell count and determination of the
levels of inflammatory markers, are both important parts of the assessment of a
patient with an acute presentation of bursitis. It is also important to not
confuse a diagnosis of septic arthritis with that of septic bursitis because
the presentation may be similar.
Treatment. In acute cases
of aseptic bursitis, improvement is commonly possible with rest, compression,
ice, and padding or protection of the involved area. Short- term immobilization
in a well-padded splint may also be utilized for a patient with an acutely
inflamed knee to prevent further irritation or stress on the bursa by excessive
range of motion or further trauma to the area. Aspiration may be beneficial for
pain relief and for diagnostic purposes in cases of septic bursitis.
Parenterally administered anti-inflammatory agents are commonly used for pain
relief as well. In chronic cases that have failed nonoperative treatment or in
cases of acute suppurative infection, surgical bursectomy is recommended. In
the case of septic bursitis, appropriate antibiotics are also an essential part
of treatment.
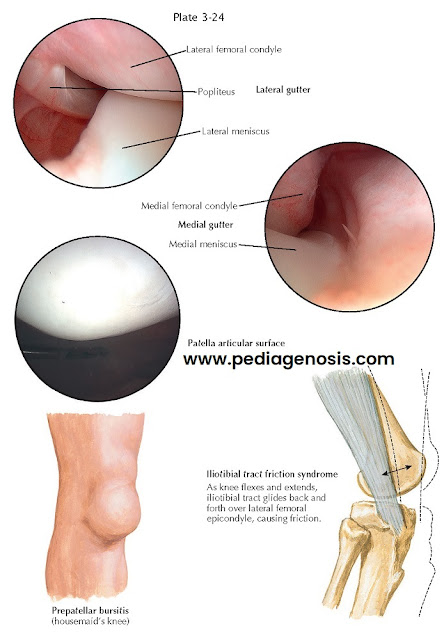
ILIOTIBIAL BAND FRICTION SYNDROME
This is a chronic inflammatory process involving the
soft tissues adjacent to the lateral femoral epicondyle, presumably caused by chronic “friction” of iliotibial
band rubbing over a bony prominence of this area. Runners are commonly affected
by this overuse-type syndrome. The patient may present with lateral knee pain
on activity, tightness of the iliotibial band, and occasionally popping.
Treatment. Initial treatment options include ilio- tibial band stretching exercises, anti-inflammatory agents, ultrasound to the lateral femoral epicondyle, and corticosteroid injection. Physical therapy protocols, particularly those including stretching regimens, are also routinely used for symptomatic patients. Rarely, in refractory cases, surgery can be done to release an area of tightness or debride any focal areas of inflammation.


.webp "SCROTAL SKIN DISEASES I : CHEMICAL AND INFECTIOUS")
